
Eric Clapton, Musician, and his Covid Vaccine Injury – Safe and Effective?
Source of Featured Image
“… ramped up from, on a scale of ten, say, from 3 to … 8 or 9 … Agony and chronic pain …”
(Go to 10:20 minutes for screenshot.)
Please note: The advertisements are NOT mine.
Dear Pain Matters readers,
Sadly, countless people suffer from severe adverse reactions including chronic pain following their experimental Covid mRNA injections including famous musician, Eric Clapton.
Quoting Eric Clapton in an interview with Robin Monotti, Italian architect and film producer, regarding his adverse reaction to the AstraZeneca injection:
“I can’t sleep because of the pain … the vaccine took my immune system and just shook it around …
… and I went and had the jab and I got a little green [card] (like a library card), and I thought that’s what I’m going to show the people when I get on the plane. … Within several hours, I was shaking like a leaf and I went to bed early and I couldn’t get warm … I thought … am I running a fever? I was boiling hot and sweating, and then I was cold. … I was out for the count for about a week.
I had been preparing for a project where I was going to be playing acoustic guitar with a couple of musicians and we were going to film it that week. Knocked me out and I had to start again from scratch. … It didn’t come off as well as I would like to … It was a huge setback and it frightened the **** out of me because I didn’t know how long it would last. I then started to find out more …
… bit by bit, I realised that I probably shouldn’t have had the first jab but then I was offered the second [jab]. I thought, well, … what’s the point in … stopping now? So I went and had the second [jab], … And then it got really bad and within about a week, I had lost my hands – [they] didn’t really work. … I suffered from a condition … called peripheral neuropathy, which is nerve damage pain, … which means that … I can get numb, or pins and needles. …
This [pain] … ramped up from, say, 3 to … 8 or 9 (on a scale of 10). Agony and chronic pain … I have gigs to do, I have recording work to do, but I can’t … play the guitar, it’s not fun and it’s something I do … then when I put [the guitar] down, [the pain] is there until I go to bed. I take sleeping pills because I can’t sleep because of the pain, and that’s … not a good way to live … the vaccine took my immune system and just shook it around again, and that’s still going on …
… and I called my … NHS doctor after the second jab and I said, “I’ve been told there’s a yellow card system … where I can complain about after-effects?“ He said … , “I’ll fill in the report …” …
I lost the use of my hands for about 3 weeks, so I thought I was in real trouble. That’s about that point I was invited by Robin Monotti to talk about it … because I realised that … I wasn’t the only one that was suffering adverse reactions … I can’t touch anything cold or hot, I have to use these [gloves], otherwise my hands will begin to burn and they’ll stay burnt all day.
… that’s my experience from having had the second jab … I went to my doctor … and said, you know, I can’t have any more vaccinations. This is not possible for me because I don’t know what will happen. I don’t know what will happen next. …”
Source:
Eric Clapton: Exclusive & Uncensored Oracle Films – Robin Monotti in conversation with Eric Clapton
(24 minutes; transcript available; 14 June 2021; 492,000 views)
https://www.youtube.com/watch?v=4OHmMKrVbNk
via https://t.me/robinmg/26449
Quoting Eric Clapton in another interview with Robin Monotti:
“In February [2021] this year, before I learned about the nature of the [Covid] vaccines and being 76 with emphysema, I was in the avant garde. I took the first jab of [AstraZeneca] and straight away, [I] had severe reactions which lasted 10 days, I recovered eventually and was told it would be 12 weeks before the second one…
About 6 weeks later, I was offered and took the second [AstraZeneca] shot, but with a little more knowledge of the dangers. Needless to say, the reactions were disastrous. My hands and feet were either frozen, numb or burning, and pretty much useless for 2 weeks. I feared I would never play again. I suffer with peripheral neuropathy and [I] should never have gone near the needle. But the propaganda said the vaccine was safe for everyone. …”
Source:
Robin Monotti: A Conversation with Eric Clapton | Oracle Films
(22-minutes; transcript available; 16 June 2021)
via https://t.me/robinmg/3377,
Thank you very much, Robin Monotti, for sharing Eric Clapton‘s experiences that will hopefully help others struggling with side effects including chronic pain, post-Covid injection.
In closing today, I leave you with 2 songs by Eric Clapton, one written in 2021 and the second one written in 1992. Like so many of his songs, the lyrics to these songs are laden with meaning hence worthwhile analysing in greater detail:
This Has Gotta Stop
…
I knew that somethin’ was goin’ on wrong
When you started layin’ down the law
I can’t move my hands, I break out in sweat
I wanna cry, can’t take it anymore
…
I’ve been around long, long time
Seen it all, and I’m used to being FREE
I know who I am, try to do what’s right
So lock me up and throw away the key
This has gotta stop
Enough is enough
I can’t take this BS any longer
It’s gone far enough
If you wanna claim my soul
You’ll have to come and break down this door
Tears In Heaven
https://www.youtube.com/watch?v=JxPj3GAYYZ0
Sabina Walker
Master in Applied Science (Neuroscience)
Blogger, Pain Matters
ADDITIONAL REFERENCES
(1) Eric Clapton: I should never have gone near the needle.
(3) Makis, William MD
Musicians Injured – Eric Clapton: “I can’t sleep because of the pain … the vaccine took my immune system and just shook it around” –
Eric Clapton bravely discusses his neurological COVID-19 vaccine injuries (11 February 2023)
https://makismd.substack.com/p/eric-clapton-i-cant-sleep-because
Which Symptoms of Long Covid after Covid-19 Injections are in fact Vaccine-Induced Injuries?
Dear Pain Matters readers,
A question that often haunts is:
When is “Long Covid” ACTUALLY caused by the experimental Covid-19 injection, hence vaccine-induced injuries (also popularized as “Post-VAC-Syndrome”)?
Renowned researchers are now asking this question more often including Associate Professor of Neurology at Harvard Medical School and Assistant in Pathology (Neuropathology), Anne Louise Oaklander (quoting):
“You see one or two patients and you wonder if it’s a coincidence … But by the time you’ve seen 10, 20 … Where there’s smoke, there’s fire.”
According to Oaklander (who is renowned for her research into small fiber neuropathy), symptoms that may appear within mere hours, days or even weeks after the Covid-19 injection may include:
- persistent headaches;
- severe fatigue; and
- abnormal heart rate and blood pressure.
Specifically, patients with post-vaccination symptoms may present with:
- Small fiber neuropathy, that involves nerve damage that can cause electric shock–like, tingling sensations, burning pain and blood circulation problems; and/or
- Small fiber neuropathy-induced postural orthostatic tachycardia syndrome (POTS), that can involve muscle weakness, unusual variations in heart rate and blood pressure, fatigue and brain fog.
More details here:
Rare link between coronavirus vaccines and Long Covid–like illness starts to gain acceptance – Studies probe unusual cases of neurologic complications, blood pressure swings, and other side effects (3 July 2023)
Sabina Walker
Blogger, Pain Matters
REFERENCES
(1) Vogel, Gretchen; Couzin-Frankel, Jennifer.
Rare link between coronavirus vaccines and Long Covid–like illness starts to gain acceptance – Studies probe unusual cases of neurologic complications, blood pressure swings, and other side effects (3 July 2023).
Science (July 2023), Vol 381, Issue 6653
(2) Another article by the same authors:
Vogel, Gretchen; Couzin-Frankel, Jennifer.
In rare cases, coronavirus vaccines may cause Long Covid–like symptoms (20/1/2022)
Science (Jan 2022), Vol 375, Issue 6579
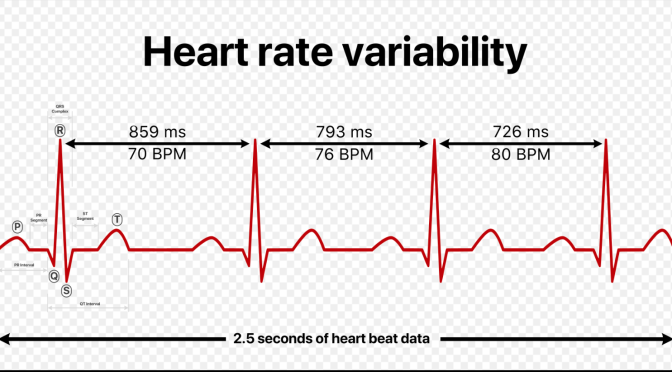
Researchers in Oslo, Norway, Explore the Relationship Between Heart Rate Variability (HRV) and Pain
Source of Featured Image
https://en.wikipedia.org/wiki/Heart_rate_variability
Dear Pain Matters readers,
Renowned heart rate variability (HRV) researchers, Associate Professor Daniel Quintana, PhD candidate Emilie Kildal and colleagues in Oslo, Norway, have recently written a science paper (not yet formally published) called:
Heart Rate Variability and Pain: A Protocol for a Systematic Review and Meta-Analysis (August 2023)
Why is this exciting?
Heart rate variability including heart rate variability – high frequency (HRV-HF) may add further objective insight into patients’ pain intensities, in addition to current diagnostic tools (that often involve subjective diagnostic tools such as pain questionnaires). For example, many patients including nonverbal patients (e.g. dementia), babies/toddlers and those with language difficulties (e.g. recent migrants) may not be able to comprehend the pain questionnaires.
Quoting from the draft science paper by Kildal, Quintana and colleagues,
“Establishing a reliable pain biomarker may significantly improve care for nonverbal patients otherwise unable to express their pain (e.g., individuals with profound autism, cerebral palsy, aphasia due to stroke, or profound intellectual disability). Amidst potential candidates, heart rate variability (HRV) has garnered growing attention. … … we aim to elucidate the association between HRV and pain. …”
Thus, Quintana and colleagues aim to explore:
– the relationship between HRV and experimentally induced pain;
and
- how chronic pain patients compare to healthy individuals with respect to HRV.
We eagerly await the findings of this Systematic Review and Meta-Analysis planned by the team headed by Daniel Quintana at the University of Oslo, Norway.
See my 2 other blog posts on HRV including why and how HRV could offer another (more objective) way to diagnose pain:
1)
2)
Sabina Walker
Blogger, Pain Matters
REFERENCES
(1) Kildal, E.S.M., … Quintana, D.S. Heart Rate Variability and Pain: A Protocol for a Systematic Review and Meta-Analysis (16 August 2023)
(2) Kildal, E.S.M., Quintana, D.S., Szabo, A. et al. Heart rate monitoring to detect acute pain in non-verbal patients: a study protocol for a randomized controlled clinical trial. BMC Psychiatry 23, 252 (2023). https://doi.org/10.1186/s12888-023-04757-1

Complex Regional Pain Syndrome (CRPS) after Experimental Covid-19 Injection

Subscribe to continue reading
Subscribe to get access to the rest of this post and other subscriber-only content.

Successful Abatacept treatment for an autoimmune disorder that causes painful and swollen joints
Source of Featured Image:
Dear Pain Matters readers,
I am sure that you will enjoy this story about Karla as much as I did!
Genome testing has changed Karla De Lautour’s life and helped scientists understand her autoimmune condition (21/5/2020)
Quoting her rheumatologist, Dr Davinder Singh-Grewal,
“[Karla] had a lot of pain [due to painful and swollen joints], she was stiff every morning and it really was affecting her ability to live a normal life.”
Enter Professor Chris Goodnow and his team at Sydney’s Garvan Institute who not only found a single fault in her genome, but also knew that an existing drug, Abatacept, could target the problem.
When Chris Goodnow met Karla for the first time (after successful Abatacept treatment), he was overjoyed to find Karla transformed into “a fantastic, chirpy, totally normal, 7-year-old”, thanks to his team’s research.
Not only does Abatacept directly target Karla’s painful autoimmune disorder, but it is also much easier for her to tolerate.
Karla now has an Abatacept infusion once every 2 weeks that offers her pain relief.
In closing, her rheumatologist said,
“Had they not sequenced the genome, [Karla] would have continued on in pain.”
Karla added,
“It feels better because it makes my pain go away and it feels comfortable.”
What could be better than this??
I hope you enjoyed this heart-warming story about Karla.
Sabina Walker
Blogger, Pain Matters (painmatters.wordpress.com)
MORE ON ABATACEPT
Abatacept (brand name Orencia) is part of a new class of medicines called biological disease modifying antirheumatic drugs (biological DMARDs or bDMARDs).
Abatacept blocks T cell (a type of white blood cell) responses. This leads to reduced inflammation, less joint damage and, best of all (from a patient’s perspective), decreased pain, swelling and other symptoms.
Abatacept is offered as a drip (infusion) into the vein. Alternatively, it is given as an injection under the skin of the abdomen or thigh (subcutaneous injection). The infusion usually takes 30 minutes. Additional doses may be given every 2 – 4 weeks after the first dose.
REFERENCES
(1) Lloyd, Mary. Genome testing has changed Karla De Lautour’s life and helped scientists understand her autoimmune condition. ABC News (21/5/2020).
(2) Abatacept. Arthritis Australia
https://arthritisaustralia.com.au/medication-search/abatacept/

Enbrel (Etanercept) for CRPS – Professional Footballer, Nazair Jones, and his CRPS Story
Feature Image of Nazair Jones, Professional Footballer, sourced from:
Dear Pain Matters readers,
Here is a patient story that may inspire, empower and offer hope.
This story is about a footballer named Nazair Jones who developed CRPS at only 15. Amongst many treatments, Nazair received regular injections of Enbrel (Etanercept) and physiotherapy. Details follow:
| As a teenager, Nazair Jones always enjoyed playing football and basketball. Unfortunately, his passion for competitive sports led to a number of injuries including torn anterior cruciate ligaments, shoulder surgeries and broken limbs.
On 5 November 2011, Nazair Jones (then 15) woke up to a body inexplicably paralyzed from his waist down. He could not get out of bed to go to the bathroom. His body was frozen in agony and he could not move his legs due to excruciating pain. Quoting Nazair, ‘On a scale of 1 to 10, the pain was a 12.’ Terrified, he yelled to his mom for help. In Nazair’s words, ‘It’s hard to explain…It was a shock…In my head, I’m saying ‘Walk. Walk! Why aren’t you walking?’ It was scary.’ Nazair’s mom called an ambulance to take him to Emergency. He was discharged shortly after receiving an injection for pain. Sadly, Nazair’s pain came back with a vengeance. He was given injections including an epidural for pain. Despite ultrasounds of his legs as well as nerve and blood tests, no one knew why Nazair had severe pain or why he could not walk. Nazair’s ankle was extremely swollen. The swelling would switch from one ankle to the other the following morning. His swollen leg would also sweat profusely even while lying down. In Nazair’s words, ‘They didn’t know what was wrong with me. That was the worst part.’ Nazair was finally diagnosed with CRPS in December 2011. He required a cane, a walker and ultimately a wheelchair for mobility. Doctors were unsure if he’d ever walk again, let alone play football again. Despite his pain including allodynia* and mobility issues, Nazair never forgot his dream of becoming a professional footballer. Motivated by his dream, Nazair started daily physiotherapy including walking exercises in the pool and mirror therapy. Despite pain medication including ibuprofen, he suffered excruciating pain. It would take Nazair an entire 30 to 60 minutes just to walk around the hospital floor. Quoting Nazair, ‘It sounds easy to take a lap, but it was, by far, the worst pain. You’re trying to get your body to do something—you want it to do it—but it’s just not doing it. You’re forcing yourself to move, and it just hurts. I can’t even explain the hurt. It just hurts … with all of that swelling, that was the most painful part …’ In 2013, Nazair started receiving weekly Enbrel (Etanercept) injections to manage the swelling in his ankles. The good news is that Nazair was finally able to walk on his own again in May. Two months later in July, he started playing sport again. In his words, ‘… I just know I’ve been able to be myself with no pain.’ (Adelson, 2016; Adelson, 2017; Dunne, 2017; Supportive Care Matters, 2018). |
Wishing all pain patients inspiration, hope and empowerment
Sabina Walker
Masters Appl. Science (Neuroscience)
Blogger, Pain Matters (in WordPress)
painmatters.wordpress.com
and
Author of soon-to-be published book called Pain Matters
@SabinaWalker18
KEY
* Allodynia is pain caused by a stimulus that is usually not painful.
REFERENCES
(1) Adelson, Andrea. UNC DL Nazair Jones was nearly paralyzed five years ago. ESPN (28 Sept 2016).
(2) Adelson, Eric. NFL draft prospect Nazair Jones on his rare disease: ‘On a scale of 1 to 10, the pain was a 12.’ Yahoo Sports (7 April 2017).
(3) Dunne, Tyler. Unable to Walk at 16, UNC Lineman Naz Jones Is About to Get Drafted into the NFL. Bleacher Report (6 April 2017).
(4) Supportive Care Matters. Nazair Jones Goes from Chronic Disease to NFL Hopeful (2018).

Surgery to Remove Schwannoma Leads to Relief from Tumour Pain in Face
Feature Image of a woman holding her face in her hands is sourced from:
https://unsplash.com/photos/CCFCMb1Defk
Dear Pain Matters readers,
When severe pain is caused by tumours, benign or cancerous, surgery including stereotactic radiosurgery to remove the tumour may be the most effective way to reduce or eliminate tumour-induced pain.
A Decade of Severe Facial Pain Caused by an Undiagnosed Tumour
Stereotactic Radiosurgery of Schwannoma Leads to Pain ReliefMichelle Ellerbe, married and mother of 2 daughters, suffered a decade of severe facial pain. Michelle’s excruciating pain started on the right side of her face in 2008 after giving birth to her second child. In her words, ‘I felt a sharp pain radiate from my right ear to my right nostril … The whole day, the pains got worse. … I went to emergency … They told me I had Bell’s palsy, gave me steroids and sent me home.’ During her next emergency room visit a week later, she undertook numerous tests including MRI, CT scan and blood tests – but still no correct diagnosis. Despite seeing countless doctors, taking ‘too many pain pills’ (ibuprofen, oxycodone, morphine, methadone and Dilaudid) and antiseizure medication and undergoing multiple surgeries and procedures (e.g. Gamma Knife procedure, nerve blocks), Michelle’s facial pain persisted more than 2 years. A doctor diagnosed trigeminal neuralgia while another doctor performed a glycerol nerve block, to no avail. A neurosurgeon performed craniotomy while an oral surgeon extracted all of her teeth on the right side of her mouth, all without success. In Michelle’s words, ‘I was broken. Everyone started saying they can’t help me, and kept giving me more medication. I was taking 22 pills a day to show up at work. … I thought I was going to die from an overdose.’ Then one day, Michelle saw Dr Philip Stieg, a neurosurgeon in New York. After diagnostic imaging, Dr Stieg found a tumour, specifically, a Schwannoma around her trigeminal nerve. Usually benign in nature, a Schwannoma is a nerve sheath tumour that develops from the Schwann cell. Whilst dismissed as ‘calcification’ on an older CT scan dated 2013, this (growing) tumour was (likely) the source of her severe facial pain for a decade. Stereotactic radiosurgery was done to eliminate the tumour. After 3 radiation therapy sessions, Michelle reduced her daily intake of pain pills from 22 to 7, and later on, a maximum of 2 pain tablets a day. Whilst Michelle still has some residual pain due to nerve damage caused by all the past surgeries and procedures, her quality of life is significantly improved. In Michelle’s words, ‘I’m off all of that medication …this summer, … I will be on a beach or sitting in a park with my family enjoying the breeze pain free!’ For more details, please see: Michelle Ellerbe’s Story NewYork-Presbyterian (2019) https://www.nyp.org/patient-stories/patient-story-michelle-ellerbe |
Summary
Tumour facial pain may be effectively treated via surgery including stereotactic radiosurgery to remove the tumour.
Wishing all pain patients inspiration, hope and empowerment
Sabina Walker
Masters Appl. Science (Neuroscience)
Blogger, Pain Matters (in WordPress)
painmatters.wordpress.com
and
Author of soon-to-be published book called Pain Matters
@SabinaWalker18

A SINGLE Perispinal Etanercept Injection by Edward Tobinick MD for Severe Nerve Pain including Sciatica and Post-Stroke Pain (2/2)
Feature Image sourced from:
Dear Pain Matters blog readers,
Introduction
Infliximab, Etanercept and other selective anti-TNF drugs are sometimes used to treat:
- Lumbar radicular pain;
- Sciatica;
- Post-stroke pain;
- Complex regional pain syndrome (CRPS);
- Rheumatoid arthritis;
- Crohn’s disease; and
- Other painful conditions.
This blog post explores the pain-relieving effects of a single perispinal Etanercept injection in certain patients with sciatica, post-stroke pain and other severe nerve pain.
An earlier blog post discussed anti-TNF drugs (Infliximab) for CRPS:
Anti-TNF Drug (Infliximab) Therapy for CRPS and Other Chronic Pain Conditions (1/2)
A Single Perispinal Etanercept Injection for Pain in Back (Sciatica), Neck and after Stroke – 9 Patient Stories
A handful of pain patient stories (N=9) were selected from the Institute of Neurological Recovery’s (INR’s) website (that has over 300 patient videos). This website also includes media stories, a blog and countless scientific publications by Dr Tobinick and his peers (see References).
Please note the following disclaimer quoted from Dr Tobinick’s Patient YouTubes:
‘Disclaimer: Individual results vary, not all patients respond. Additional doses may be necessary to maintain the clinical response. Treatment for these indications is innovative (“off-label”). The method of off-label treatment utilized is a patented invention of the INR®.’
(1) Kerry and Her Single Perispinal Etanercept Injection for Severe Leg and Back Pain‘Kerry’ (not her real name) had intense right ankle, leg and back pain including burning pain for 6 months nonstop. She walked very slowly with an abnormal gait to prevent the pain from shooting down her leg. Her sleep was severely compromised. Kerry was offered a single dose of perispinal Etanercept by Dr Tobinick at the Institute of Neurological Recovery, Florida, on 11 September 2009. Kerry was immediately pain free at rest! When her right leg was gently lifted, there was only a little pain. She said that this was likely due to not doing enough stretching exercises. Kerry did not have pain in her buttocks nor lower back and her gait was vastly improved. In Kerry’s words, ‘I feel good! Thank you. Yeah, I feel good.’ At her follow-up 2 weeks later on 25/9/2009, Kerry said that she felt excellent. She slept well and was able to do all her normal activities. Kerry attributed her complete recovery from pain and mobility to her single dose of Etanercept. For more details, please view Immediate and sustained relief from severe pain (a 4-minute YouTube dated 25/11/2009 by the Institute of Neurological Recovery, Florida). |
(2) Ana and Her Single Perispinal Etanercept Injection for Severe Back and Leg Pain‘Ana’ (not her real name), a woman with a warm Spanish accent, suffered constant severe back and leg pain for 2 years. Ana’s unrelenting pain affected her mobility and sleep. Her husband had to help put on her shoes and underwear. Ana tried different pain medications including Tramadol, Vicodinand Naproxen without success. Ultimately,Ana lost her job because of her ongoing pain. Ana booked an appointment with Dr Tobinick at the Institute of Neurological Recovery, Florida, on 4 May 2009. While seated during the examination, Ana’s left leg was gently raised. This resulted in increased pain in her back that spread down her left leg. It was impossible to lift her other leg due to excruciating pain. Thereafter, Ana received a single dose of perispinal Etanercept. Three minutes afterward, Dr Tobinick stated, ‘All right now. … The dose was at 9 minutes after 4, and this … is 3 minutes [later]. What is happening?’ Ana said, ‘I can move my legs! [She laughs, with tears of joy in her eyes.] Oh God! Oh God!’ Dr Tobinick asked, ‘Is this different?’ ‘Oh yeah!’, she exclaimed. He continued, ‘When was the last time you felt like this?’ Ana replied, ‘I don’t know, about 2 or 3 years ago. Oh my God! … I can’t believe this! Two years of pain … Oh my God! Wow! You’ve given my life back! Dr Tobinick asked, ‘What do you think?’ She tearfully said, ‘Thank you!’ Dr Tobinick continued, ‘How do your legs feel? … Before, it was hurting.’ She happily replied, ‘Oh, thank you … I have legs!’ He added, ‘Can you walk?’ She said, ‘Oh my God!’ Dr Tobinick said, ‘How do you feel? Let’s go down the hall.’ Ana said, ‘Oh my God! … This is incredible! Oh God.’ He asked, ‘Did it work?’ She enthusiastically replied, ‘Yes!! … Thank you so much!’ Ana (and her husband) had a follow-up visit with Dr Tobinick a week later on 11 May 2009. Ana’s husband exclaimed, ‘… This is another person. That was not her … I got her back! … The smile! … She’s alive! … She’s getting back into the game … She’s moving!’ Ana had another follow-up visit with Dr Tobinick 3 months later on 14 August 2009. Dr Tobinick asked, ‘What kind of difference has this [single dose of perispinal Etanercept] made for your life?’ Ana replied, ‘Tremendous! … I’m holding my grandson and playing with him … I can have him in my lap and play with him. … And enjoy it! I wasn’t able to do that before! I’m doing a lot better!’ Dr Tobinick said, ‘Wonderful!’ ‘Thank you, Dr Tobinick!’ ‘You’re welcome!’ For more details, please view Immediate relief of 2 years of constant back pain and sciatica (an 8-minute YouTube dated 25/11/2009 by the Institute of Neurological Recovery, Florida). |
(3) Brenda’s Single Perispinal Etanercept Injection Brings Fast Relief from Severe SciaticaA young woman named ‘Brenda’ (not her real name) had a slipped disc in her 4th vertebra and severe sciatic pain for 5 months since December 2008. Her gait was affected and she had severe pain from the right side of her lower back and buttocks that spread down both legs. There was unbearable pain in her right leg down to her toes and less pain in her left leg. Brenda was given Vicodin, steroids and morphine injections for her pain, to no avail. When she was rushed to hospital for severe back pain (several times), the neurosurgeon told her that she needed emergency back surgery. When Brenda went to see Dr Tobinick on 21 April 2009, he confirmed that the pain on the right side of Brenda’s back worsened when her left leg was lifted. Thereafter, Brenda was offered a single dose of perispinal Etanercept. Within only 1 minute after her injection, Brenda’s knee no longer hurt! There was no pain in her back even as she lifted both legs. When she stood up to walk around, there was nil pain and her gait was normal. Happy to finally be pain free, she started dancing! When asked by Dr Tobinick, ‘How much pain do you have?’ She replied, ‘I don’t have any pain!’ He confirmed, ‘Your pain is all gone?’ She answered cheerfully, ‘I’m not in pain! Nope, I’m not in pain! Nope! I’m good! Before, I couldn’t stand on this leg … I feel good! I feel great!’ For more details, please view Rapid relief after 5 months of severe sciatic pain (a 5-minute YouTube dated 7 Jan 2016 by the Institute of Neurological Recovery, Florida). |
(4) Tim’s Single Perispinal Etanercept Injection Offers Relief from Sciatica in Minutes‘Tim’ (not his real name) went to see Dr Tobinick on 4 April 2007 for severe sciatica. The intense pain was constant and unbearable for 3 weeks and affected his work, quality of life and sleep. He had pain in his back and buttocks that extended down his left leg to his calf. In Tim’s words, ‘It feels like somebody took a baseball bat and hit my leg.’ The pain increased in Tim’s left (not right) leg when Dr Tobinickgently moved his right leg. Tim’s pain was more intense when seated and it lessened when he stood up. He was able to walk ‘with a slight limp but real slow … real gently’. Tim had pain relief within a 1 minute after Dr Tobinickinjected Etanercept perispinally. In response to Dr Tobinick’s question about how he was feeling right after the injection, Tim replied, ‘[The pain] feels kind of pulsating right now … down my leg. It’s not a constant pain like it was.’ Dr Tobinick replied, ‘… So [the pain has] changed in character a little bit … already’ ‘Correct,’ Tim replied. ‘I feel it in my butt still but not down the leg.’ Dr Tobinick confirmed, ‘But you feel it in your lower back and in your butt?’ ‘Correct.’ Dr Tobinick continued, ‘But you’re starting to feel a little bit more comfortable … in general?’ ‘Yeah…yes!’ ‘… And your leg?’ ‘It’s a miracle. It’s amazing.’ ‘You’re walking a lot faster … Wow!’ Tim replied, ‘Yeah I’m loving this stuff. Once again, it worked!’ Dr Tobinick phoned Tim 3 months later on 3 July 2007 to follow up. ‘I’m wondering now how you’re feeling?’ Tim replied, ‘I am feeling like a million bucks, doctor!’ Pleased for his patient, Dr Tobinick said, ‘I love it!’ Tim continued, ‘… By the time I got back to UCLA that day [of the perispinal Etanercept injection], I was better … You would have never known I had a back problem! …’ Dr Tobinick said, ‘That’s fantastic! … You know, you had some very interesting findings. That finding of moving your right leg, making your left leg hurt, that’s a very specific finding that indicates inflammation of the nerve root. And so, it was clear what we were treating. And that, of course, got better, very quickly … So, it’s very interesting, scientifically … You’re better, and you didn’t have to have surgery!’ Tim replied, ‘Yes, I am too. That’s wonderful stuff you got there.’ For more details, please view Improvement within minutes in sciatica (an 8-min YouTube dated 12 Nov 2009 by the Institute of Neurological Recovery, Florida). |
(5) Gerry’s Single Perispinal Etanercept Injection Offers Pain Relief in Minutes after 5 Years of Sciatica‘Gerry’ (not his real name) suffered from sciatic pain for 5 years nonstop. In his words, he had pain ‘every day, all day’. Gerry tried different treatments including chiropractic and decompression treatments. Dr Tobinick treated Gerry for sciatica via a single dose of perispinal Etanercept. It took ‘just a few minutes’ for the Etanercept to offer lasting pain relief (as confirmed at the follow-up 2 weeks later on 9 July 2009). For more details, please view Relief in minutes after 5 years of constant pain (a 1-min YouTube dated 6 January 2016 by the Institute of Neurological Recovery, Florida). |
(6) Mirabelle has Improved Hand Strength After A Single Dose of Perispinal Etanercept‘Mirabelle’ (not her real name) suffered ongoing and never-ending severe pain for 15 years. Walking and standing up caused pain in her hips and low back. Mirabelle had pain in both hands. Her left hand was weaker and more painful than her right hand ever since her ski accident in 1986 or 1988. Mirabelle was seen by nearly 30 different doctors including 10 or 11 pain specialists. During her appointment with Dr Tobinick, Mirabelle received asingle dose of perispinal Etanercept. When followed up 2 weeks later on 24 October 2007, Mirabelle had significantly more strength in both hands, compared to before Etanercept injection. Her hands no longer had ‘that arthritic feeling’ (that she felt for weeks). While there was some residual muscular pain, Mirabelle no longer had neck pain, post-Etanercept. For more details, please view Hand improvement after treatment at the INR in 2007 (a 6-min YouTube dated 6 January 2016 by the Institute of Neurological Recovery, Florida). |
(7) Caroline’s Sole Perispinal Etanercept Injection Relieves 25-Year Pain in 10 MinutesAt follow-up on 15 July 2009, 2 weeks after ‘Caroline’s’ (not her real name) single injection of perispinal Etanercept, Dr Tobinick asked, ‘What happened [after this injection]?’ Caroline replied, ‘… I got up … I felt … so much taller … I felt … this wonderful feeling … I stood up and it was just great … I was elated because Ihave been in pain for sooo long … [The pain was] like a knife going through you …’ Dr Tobinick continued, ‘And how long did you have the pain?’ Caroline answered, ‘Oh, I’ve had the pain … I started maybe 25 years ago …’ He asked, ‘How long?’ Caroline clarified, ‘This has been the worst, these last few years. … The last 4 years.’ Dr Tobinick asked, ‘Have you had it every day?’ She replied, ‘Just about!’ He continued, ‘Just about every day? And how many hours a day were you having the pain before you came in?’ Caroline answered, ‘Oh gosh, very, very often.’ He clarified, ‘So most of the day? …’ Caroline stated, ‘And this time when I had that injection, it’s unbelievable.’ ‘How long did it take to work?’ he asked. ‘10 minutes!’ ‘10 minutes,’ he confirmed. She said, ‘Unbelievable. It is. It really is! Dr Tobinick asked, ‘Has anything like this happened at all in the last few years?’ ‘No. [Not] at all,’ she replied. ‘It’s incredible. I really did not believe this could happen …’ Dr Tobinick asked, ‘Have you had to take any pain medicine in the last 2 weeks?’ ‘No,’ she answered. ‘Not a single … no pills? Nothing?’ he confirmed. ‘Nothing! ‘Ok,’ he said. ‘It’s really great! …’, she said. ‘…I’ve had … surgery … I got worse.’ Dr Tobinick asked, ‘You had surgery for your back?’ ‘Yes!’ ‘And you got worse?’ ‘And I got worse … And yet I come to this, and it’s great! … It’s the greatest thing that’s come along. …’ ‘… Alright, thank you very much,’ Dr Tobinick said. For more details, please view the 4-minute video called Rapid pain relief after 25 years of pain July 15, 2009 (a 4-min YouTube dated 6 January 2016 by the Institute of Neurological Recovery, Florida). https://www.youtube.com/watch?v=3ClVijm0MAA&feature=youtu.be&app=desktop |
(8) Lola and Her Single Perispinal Etanercept Injection for Post-Stroke Pain‘Lola’ (not her real name) suffered ongoing severe pain for almost 2 years after a stroke on 27 November 2016. Her excruciating pain (10/10) affected the entire left side of her body including arm, breast, ribs, hip and leg. She rarely moved her left arm nor left foot due to extreme pain. Walking was next to impossible as her pain would only intensify with activity. Lola tried Baclofen and Gabapentin for pain without success. Lola booked an appointment with Dr Edward Tobinick on 20 November 2018, almost 2 years after her stroke. After an assessment, Lola received a single perispinal Etanercept injection. Lola enjoyed immediate pain reliefand improved left arm mobility within 10 minutes after her injection. Her pain levels in her chest dropped to 6/10. Lola was finally able to move her left arm without pain. The spasticity in her left arm was also reduced. Lola no longer had hip pain (that was 10/10 prior to injection). The pain in her left leg and foot was gone, she was able to move her left foot for first time in 2 years and her balance was significantly improved. Lola finally took her first steps without pain. Overall, Lola enjoyed significantly less pain and enhanced mobility thanks to her single Etanercept injection. According to her daughter, there was a new look in Lola’s eyes. When Dr Tobinick asked, ‘Are you happy you’ve come?’, Lola replied, ‘I’m very happy … And I hope I give hope to other patients too!’ For further details, please view Immediate improvement in chronic post-stroke pain nearly 2 years after stroke (a 3-minute YouTube dated 28/11/2018 by the Institute of Neurological Recovery, Florida). |
(9) Debbie and Her Single Perispinal Etanercept Injection for Post-Stroke Pain‘Debbie’ (not her real name) had a massive stroke that led to mobility issues and severe, unrelenting pain in her neck, both shoulders and upper left arm. While strong pain medication reduced some of her pain, it did not eliminate it. Debbie was unable to get out of a chair without assistance and she required a wheelchair during shopping. She had significant loss of function in her left hand and arm as well as loss of sensation in the left side of her body including face, hand and leg. Debbie had her first appointment with Dr Tobinick 3 years after her stroke on 29 February 2012. Dr Tobinick asked, ‘Do you have pain every day?’ ‘Yes, every minute of every day, I’ve got pain.’ Dr Tobinick confirmed, ‘Every minute of every day? You have constant pain?’ ‘Yes’, she replied. ‘Even now, you’re in pain?’, he asked. ‘Yes, I am…’ Within only minutes after a single perispinal Etanercept injection, Debbie had significantly less pain and restored sensation to the left side of her body including face, hand and leg. The motor skills in her left hand were dramatically enhanced and she was finally able to get out of a chair without assistance. ‘How different is that from before?’ ‘I can’t believe it. It’s a miracle!’, she said with a big smile. It’ll change my life totally!’ For further details, please view Rapid improvement in chronic post-stroke pain 3 years after stroke (a 4-minute YouTube by the Institute of Neurological Recovery, Florida). |
Perispinal Etanercept Injections for Pain due to Bone Metastasis – Case Study (N=2)Two patients received perispinal Etanercept injections near the site of bone metastases for pain. This treatment led to (quoting) ‘rapid, substantial, and sustained relief of chronic refractory pain at the treatment site’ in both patients (Tobinick, 2003). |
Perispinal Etanercept Injections for Chronic Back and/or Neck Disc-Related Pain – A Study (N=143)A study was done involving perispinal Etanercept injections into the spine of 143 patients with chronic back and/or neck disc-related pain. This treatment led to significant reductions in pain, sensory dysfunction and weakness (Tobinick and Davoodifar, 2004). |
An Australian Trial involving Perispinal Etanercept Injections for StrokeInspired by the outstanding results achieved after a single perispinal Etanercept injection by Dr Tobinick at the Institute of Neurological Recovery (INR), Florida, a clinical trial is now underway for stroke patients in Australia. Quoting, ‘The project will enable more Australians of working age who have had a stroke to access new … treatment options to aid their recovery.’
While results are not yet finalised, further details are here:
http://www.nrimed.com/wp-content/uploads/GH134.pdf
|
Summary
More research into anti-TNF drug treatment for CRPS, sciatica, post-stroke pain and other nerve pain conditions is encouraged. Such studies should confirm whether localised TNF levels are elevated in CRPS-affected limbs and other pain-affected areas in the first place. If yes, analysis is necessary whether any anti-TNF drug treatment leads to a significant reduction in these elevated localised TNF levels, and if yes, whether this is also accompanied by reduced pain (etc). Induced skin blisters or skin biopsies may be necessary to confirm localised TNF levels in CRPS-affected limbs and other pain-affected regions, both ‘before’ and ‘after’ anti-TNF drug treatment.
NOTE: If localised TNF levels are already low to begin with (prior to anti-TNF drug treatment), anti-TNF drug treatment is (likely) not indicated.
Possible adverse effects also need to be considered prior to anti-TNF drug treatment. Medical supervision is always advised.
Wishing all pain patients less pain,
Sabina Walker
Masters Appl. Science (Neuroscience)
Blogger, Pain Matters (in WordPress)
painmatters.wordpress.com
and
Author of soon-to-be published book called Pain Matters
@SabinaWalker18
For more information about Dr Tobinick’s treatment involving perispinal Etanercept for nerve pain, please see:
Patient videos (N=307) by the Institute of Neurological Recovery, Florida:
https://www.nrimed.com/videos-by-category/
https://www.nrimed.com/videos-by-category/back-neck-pain/
https://www.nrimed.com/videos-by-category/stroke-pain-videos/
Scientific publications by Dr Tobinick and his peers:
https://www.nrimed.com/inr-scientific-publications/
Media stories:
http://www.nrimed.com/about/media-stories/
Blog by the Institute of Neurological Recovery, Florida:
Please note that treatment involving perispinal Etanercept injection is protected by multiple patents owned by Edward Tobinick MD including U.S. patents 6 015 557; 6 177 077; 6 419 944; 6 537 549 and Australian patent 758 523 (Tobinick and Davoodifar, 2004).
PS YOU DON’T HAVE TO READ THE FOLLOWING UNLESS YOU ARE INTERESTED IN THE UNDERLYING SCIENCE
POSSIBLE MECHANISMS OF ANTI-TNF DRUG THERAPY IN CRPS NERVE PAIN
Anti-TNF drugs (e.g. Infliximab, Etanercept) are TNF monoclonal antibodies that selectively block TNF, hence limiting the pro-inflammatory process.
The reduction of TNF and other pro-inflammatory mediators (via anti-TNF drug therapy or otherwise) may alleviate certain painful symptoms in CRPS, sciatica, post-stroke pain and other severe nerve pain conditions.
Ongoing trials are warranted including analysis of side effects.
For further details, please refer to all papers by Edward Tobinick MD and his peers.
Other papers are also available in the References including 24-page Review Paper by Sabina Walker and Prof. Peter Drummond. In particular, please see pages 1790 – 1791, plus related references on page 1804 (included below).
REFERENCES
Selected Scientific Publications by Dr Tobinick and His Peers
https://www.nrimed.com/inr-scientific-publications/
(1A) Ignatowski TA et al. Perispinal Etanercept for Post-Stroke Neurological and Cognitive Dysfunction: Scientific Rationale and Current Evidence.CNS Drugs(August 2014); 28(8): 679-697.
(1B) Tobinick E and Davoodifar S.Efficacy of etanercept delivered by perispinal administration for chronic back and/or neck disc-related pain: a study of clinical observations in 143 patients. Davoodifar S. Curr Med Res Opin(July 2004); 20(7): 1075-85.
https://www.ncbi.nlm.nih.gov/pubmed/15265252
(1C) Tobinick, Edward et al. Immediate Neurological Recovery Following Perispinal Etanercept Years After Brain Injury. Clin Drug Investig(May 2014); 34(5): 361-6.
https://www.ncbi.nlm.nih.gov/pubmed/24647830
(1D) Tobinick, Edward et al.On Overcoming Barriers to Application of Neuroinflammation Research. In: Abreu GEA, ed. Mechanisms of Neuroinflammation: InTechOpen; 2017.
https://www.nrimed.com/wp-content/uploads/Chapter7.overcoming.barriers.pdf
(1E) Tobinick, Edward. Perispinal Delivery of CNS Drugs. CNS Drugs (2016); 30(6): 469-80.
https://www.ncbi.nlm.nih.gov/pubmed/27120182
(1F) Tobinick, Edward. Perispinal etanercept advances as a neurotherapeutic.Expert Review of Neurotherapeutics (2018); 1-3.
https://www.nrimed.com/wp-content/uploads/Perispinal-etanercept-advances-as-a-neurotherapeutic-1.pdf
(1G) Tobinick, Edward. Perispinal etanercept: a new therapeutic paradigm in neurology.
Expert Review of Neurotherapeutics (June 2010); 10(6): 985-1002.
https://www.strokebreakthrough.com/wp-content/uploads/PSE.ERN2_2.pdf
(1H) Tobinick, Edward. Perispinal etanercept for neuroinflammatory disorders.Drug Discovery Today(Feb 2009); 14(3-4): 168-77.
https://www.ncbi.nlm.nih.gov/pubmed/19027875
(1I) Tobinick, Edward et al.Perispinal Etanercept for Traumatic Brain Injury.Chapter 7, pp. 109-29, in New Therapeutics for Traumatic Brain Injury, Cambridge, Mass.: Academic Press. 2017.
https://www.sciencedirect.com/science/article/pii/B9780128026861000079
(1J) Tobinick, Edward et al.Rapid intracerebroventricular delivery of Cu-DOTA-etanercept after peripheral administration demonstrated by PET imaging. BMC Res Notes(27 Feb 2009); 2: 28.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2651903/pdf/1756-0500-2-28.pdf
(1K) Tobinick, Edward L. Targeted etanercept for treatment-refractory pain due to bone metastasis: two case reports. Clinical Therapeutics. (Aug 2003); 25(8): 2279-88.
https://www.ncbi.nlm.nih.gov/pubmed/14512134
(1L) Tuttolomondo et al.Studies of Selective TNF Inhibitors in the Treatment of Brain Injury from Stroke and Trauma: A Review of Evidence to Date. Drug Design, Development and Therapy(Nov 2014); 8: 2221-2239.
https://www.ncbi.nlm.nih.gov/pubmed/25422582
Other Scientific Publications
(2) Karppinen et al; Tumor necrosis factor-alpha monoclonal antibody, infliximab, used to manage severe sciatica. Spine 2003;28:750–4.
(3) Manning; New and emerging pharmacological targets for neuropathic pain. Curr Pain Headache Rep 2004;8:192–8.
(4) Korhonen et al; The treatment of disc-herniation-induced sciatica with infliximab: One-year follow-up results of FIRST II, a randomized controlled trial. Spine 2006;31:2759–66.
(5) Burnett, Day; Recent advancements in the treatment of lumbar radicular pain. Curr Opin Anaesthesiol 2008;21:452–6.
(6) Cohen et al; Randomized, double-blind, placebo-controlled, dose-response, and preclinical safety study of transforaminal epidural etanercept for the treatment of sciatica. Anesthesiology 2009;110:1116–26.
(7) Lipsky et al; Infliximab and methotrexate in the treatment of rheumatoid arthritis. Anti-tumor necrosis factor trial in rheumatoid arthritis with concomitant therapy study group. N Engl J Med 2000;343:1594–602.
(8) Emery, Buch; Treating rheumatoid arthritis with tumor necrosis factor alpha blockade. BMJ 2002; 234:212–213.
(9) Blam et al; Integrating anti-tumor necrosis factor in inflammatory bowel disease: current and future perspectives. Am J Gastroenterol 2001;96:1977–1997.
Scientific Publication by Sabina Walker (Blogger of Pain Matters) and Professor Peter Drummond
(10) Sabina Walker, Peter D. Drummond; Implications of a Local Overproduction of Tumor Necrosis Factor-α in Complex Regional Pain Syndrome [Review Paper, 24 pages]; Pain Medicine (Dec 2011), 12 (12), 1784–1807.
In particular, please refer to pages 1790 – 1791, plus related references on page 1804 (also listed above).
http://onlinelibrary.wiley.com/doi/10.1111/j.1526-4637.2011.01273.x/abstract

Can Aromatase Inhibitors and/or Surgery Relieve Endometriosis in Women?
Feature Image of artistic depiction of female pelvic area in pain due to endometriosis sourced from:
https://theheartysoul.com/endometriosis-heart-disease-risk/
Dear Pain Matters readers,
JESSICA HIRST, ENDOMETRIOSIS SUFFERER FOR 17 YEARS, WIFE AND MOTHER
Hearing about women like Jessica Hirst inspired me to write this blog post today:
Jessica Hirst (28), a mother of a baby boy, has endured severe pelvic pain due to aggressive endometriosis since she was 11 when her periods started.

Jessica and her family
Source: https://www.mamamia.com.au/endometriosis-stories/
Quoting Jessica:
‘It feels like someone is stabbing me repeatedly in the abdomen. I get a constant burning pain. There’s an aching that starts in my lower back and comes right down through my legs … it feels like there’s a bowling ball in my uterus.’
Unable to work due to pain, Jessica relies on her husband as her full-time carer. Despite her excruciating pelvic pain, Jessica finds joy and happiness in their 18-month old baby boy. Jess is urgently in need of treatment.
Source: ‘It’s like someone’s stabbing me in the abdomen.’ – Jessica has been in pain since she was 11 (by Gemma Bath, 18 April 2019).
https://www.mamamia.com.au/endometriosis-stories/
OVERVIEW
Endometriosis is a painful disorder that affects up to 10% of all women of child-bearing age. This includes approximately 1.5 million women in the UK and 176 million women worldwide.
Furthermore, 71% to 87% of all women with chronic pelvic pain plus 38% of all infertile women have endometriosis.
Endometriosis occurs when the tissue similar to the lining inside the uterus (i.e. endometrium) grows outside of the uterus. This tissue may be found on the ovaries, fallopian tubes, tissue lining the pelvis (i.e. pelvic peritoneum), ureter, bladder, bowel and recto-vaginal septum. It has even been found in the lungs and diaphragm in rare instances.
Endometriosis can cause severe pelvic pain during periods, ovulation and/or sex. Heavy and/or irregular menstrual cycles, infertility, low energy levels, poor sleep and fatigue result. Symptoms vary depending on where the rogue endometrium grows. This can affect the women’s overall health and well-being (Amsterdam et al, 2005).
DIAGNOSIS AND TREATMENT OPTIONS
Diagnosis
Women often suffer years of pain before they are finally diagnosed with endometriosis. It takes 7.5 years on average before endometriosis is diagnosed. This is because the pain and other symptoms are all-too-often dismissed as ‘normal’ and ‘not serious’.
Endometriosis is diagnosed via biopsy obtained during diagnostic laparoscopy. This involves keyhole surgery under general anaesthetic.
Treatment Options
Endometriosis is said to be incurable (Howarth, 2019) …
… but is this always true?? Read on…
Several treatments exist that may offer relief from pelvic pain due to endometriosis:
- Oral contraceptives;*
- Aromatase inhibitors (e.g. letrozole, anastrazole); and
- Surgery (excision) to remove endometrial tissue that grows outside of the uterus.
Whilst excision of endometriosis may offer pain relief in some women, multiple surgeries may be required. Furthermore, there is a risk of recurrence. Finally, surgery is more invasive than treatment involving aromatase inhibitors.
Studies suggest that aromatase inhibitors (e.g. letrozole; anastrazole) may reduce masses hence leading to relief from pelvic pain due to endometriosis.
Aromatase inhibitors have been used to treat postmenopausal breast cancer patients for over 10 years.
SUCCESSFUL STUDIES AND CASES INVOLVING AROMATASE INHIBITORS FOR PELVIC PAIN AND ENDOMETRIOSIS
(1) An American Study (N=10) Involving Aromatase Inhibitors (Letrozole)
An American study found that aromatase inhibitors (letrozole) significantly reduced pelvic pain due to endometriosis in 9 of 10 patients.
Ten (10) premenopausal patients with endometriosis who had undergone surgical and medical treatment were selected for this study.
Endometriosis was confirmed via biopsy obtained during diagnostic laparoscopy.
Oral treatment of letrozole, together with norethindrone acetate, calcium citrate (to minimize bone loss) and vitamin D (to strengthen bones), was offered daily for 6 months.
Second-look laparoscopy was done following letrozole treatment for 6 months.
The good news:
This 2nd biopsy showed nil endometriosis in all 10 patients. Nada!
Furthermore, pelvic pain due to endometriosis was significantly reduced in 9 out of 10 patients following letrozole treatment for 6 months. Bone density appeared unaffected.
In conclusion, letrozole may offer effective treatment for endometriosis (Ailawadi et al, 2004).
(2) A 2nd American Study (N=15) Involving Aromatase Inhibitors (Anastrazole)
A 2nd American study led by the same doctor revealed that another aromatase inhibitor called anastrazole also decreased pelvic pain due to endometriosis.
Fifteen (15) premenopausal patients with endometriosis and pelvic pain were selected for this study.
Oral treatment of anastrazole and oral contraceptive was offered daily for 6 months. Anastrazole treatment led to suppression of estradiol levels.
The good news:
Fourteen of 15 endometriosis patients obtained significant pain relief following 6 months of anastrazole treatment. Specifically, median pain levels were reduced by 55% while mean pain scores were decreased by 40%.
In conclusion, anastrazole may offer effective treatment for endometriosis (Amsterdam et al, 2005).
(3) A Young Italian Woman with Endometriosis Finally Found Relief from Severe Pelvic Pain Thanks to Letrozole (After Ovariectomy Failed to Offer Pain Relief)
A young Italian woman named ‘Maria’ (not her real name) with aggressive endometriosis finally found relief from severe pelvic pain thanks to daily oral aromatase inhibitor (letrozole) treatment for 9 months.
Maria had initially undergone a subtotal hysterectomy as well as removal of both ovaries in an unsuccessful bid to reduce pelvic pain.
Following 3 months of daily oral letrozole treatment, Maria’s pelvic pain including pain during sex was significantly reduced. Her pelvic ultrasound showed nil endometrial tissue in the pelvis. Maria’s bone density remained unchanged thanks to daily calcium and Vitamin D supplements.
Given these encouraging results, treatment was continued for another 6 months.
In summary, daily oral aromatase inhibitor (letrozole) treatment may relieve severe pain in young women with endometriosis (Razzi et al, 2004).
(4) The First Woman to be Successfully Treated for Endometriosis via an Aromatase Inhibitor (Anastrozole)
An American woman (57) named ‘Jane’ (not her real name) with aggressive postmenopausal endometriosis finally found relief from severe pelvic pain thanks to daily oral aromatase inhibitor (anastrozole) treatment for 9 months.
Jane had previously undergone a hysterectomy as well as removal of her ovaries and fallopian tubes.
Guess what happened next?
Jane’s pelvic pain completely vanished after 2 months of daily oral anastrozole treatment!
Furthermore, a large 30mm X 30mm X 20mm bright red vaginal lesion had reduced to a mere 3mm gray tissue after 9-month anastrozole treatment.
Bone density was however decreased by 6.2% following 9 months of aromatase inhibitor treatment.
Aromatase inhibitors may offer benefits including pain relief and substantial eradication of endometrial tissue (
(5) Two Sisters Successfully Treated for Severe Endometriosis via an Aromatase Inhibitor (Anastrozole)
Two sisters, aged 24 and 26, had undergone several minimally invasive surgeries (i.e. laparoscopies) that, unfortunately, failed to alleviate severe pelvic pain due to aggressive endometriosis.
Both women received oral aromatase inhibitors (anastrozole), oral contraceptives (for birth control), calcitriol (to minimise bone loss) and rofecoxib (for pain control) on a daily basis for 21 days followed by 7 days off (i.e. a cycle). Six cycles were offered over 6 months.
Within only 3 months, pelvic pain and other symptoms of endometriosis were eliminated in both sisters. These positive effects lasted over a year, post-treatment.
There was nil evidence of endometriosis disease in one of the 2 sisters, as confirmed via laparoscopy done 15 months after treatment.
Bone densities remained normal in both sisters after treatment (Shippen & West, 2004).
(6) A Woman (55) Successfully Treated for Endometriosis via an Aromatase Inhibitor (Letrozole)
‘Joan’ (55) in Belgium (not her real name) underwent a total abdominal hysterectomy 10 years earlier.
Recently, Joan had right-sided sciatic pain that radiated down her right leg due to recurring endometriosis.
A pelvic ultrasound confirmed an endometrial mass that compressed against her lumbo-sacral plexus. This mass was 4cm X 8cm in size.
A daily oral aromatase inhibitor (letrozole) was offered to treat this large mass.
After 12 months of letrozole treatment, Joan no longer had sciatic pain. Following 18 months of treatment, Joan’s mass had shrunk to only 1cm in size.
Due to a successful outcome, oral letrozole was stopped after 21 months.
Recurring endometriosis may successfully be treated via an aromatase inhibitor (letrozole). This is a less invasive treatment option than surgery (Fatemi, 2005).
THE SCIENCE BEHIND ENDOMETRIOSIS AND AROMATASE INHIBITORS
An enzyme called aromatase is important in oestrogen production. This enzyme is absent in normal endometrium in the uterus.
However, this enzyme is aggressively produced in endometriosis, an oestrogen-dependent disease. Increased aromatase activity leads to high estradiol levels in endometriosis.
Being potent oestrogen blockers, aromatase inhibitors ‘starve’ endometrial tissue of oestrogen. This leads to shrinkage, and in some cases, complete elimination of endometriosis.
Thus, in the presence of aromatase inhibitors (that block oestrogen production), endometriosis may shrink, and even vanish altogether, during daily letrozole or anastrazole treatment for a certain period of time.
Aromatase inhibitors exert their anti-oestrogen effects on ovaries and on endometrial tissue growing outside of the uterus (Bulun et al, 2001; Ailawadi et al, 2004; Bulun et al, 2004; Amsterdam et al, 2005; Fatemi, 2005).
SUMMARY
In addition to oral contraceptives* and excision, aromatase inhibitors (e.g. letrozole, anastrazole) may offer effective treatment for endometriosis (Ailawadi et al, 2004; Amsterdam et al, 2005; Hofmann-Werther)
Isn’t this exciting?
If you know someone with endometriosis, please forward this blog post to her.
Wishing all pain patients inspiration, hope and empowerment,
Sabina Walker
PS From a patient’s perspective, Gabrielle Jackson’ book called Pain and Prejudice offers enormous insight into endometriosis (Jackson, 2019).
Sabina Walker, Masters Appl. Science (Neuroscience)
Blogger of Pain Matters (in WordPress)
painmatters.wordpress.com
and
Author of soon-to-be published book called Pain Matters
@SabinaWalker18
REFERENCES
MEDIA
(1) Howarth, Angus. Lack of cash hinders research into condition affecting 10% of women. The Scotsman (8 April 2019).
(2) Facts about endometriosis.
http://endometriosis.org/resources/articles/facts-about-endometriosis/
(3) Bulun, Serdar & Wood, Ros. Aromatase in endometriosis.
http://endometriosis.org/resources/articles/aromatase/
* (4) Endometriosis in adolescence. Women’s Health Queensland
https://womhealth.org.au/conditions-and-treatments/endometriosis-adolescence
(5) Hofmann-Werther, Amelie. Chronic pelvic pain and endometriosis. Middle East Medical.
https://www.middleeastmedicalportal.com/chronic-pelvic-pain-and-endometriosis/
BOOK
(1) Jackson, Gabrielle. Pain and Prejudice – A Call to Arms for Women and their Bodies. Allen & Unwin (2019).
ISBN 978 1 76052 909 3
PEER-REVIEWED PAPERS
(1a) Amsterdam et al. Anastrazole and oral contraceptives: a novel treatment for endometriosis. Fertility and Sterility (Aug 2005); 84(2), 300–304.
doi: https://doi.org/10.1016/j.fertnstert.2005.02.018
https://www.fertstert.org/article/S0015-0282(05)00859-9/fulltext
(1b) Ailawadi et al. Treatment of endometriosis and chronic pelvic pain with letrozole and norethindrone acetate: a pilot study. Fertility and Sterility (Feb 2004); 81(2): 290–296.
doi: https://doi.org/10.1016/j.fertnstert.2003.09.029
https://www.fertstert.org/article/S0015-0282(03)02874-7/fulltext
(1c) Bulun et al. Aromatase and endometriosis. Semin Reprod Med (Feb 2004); 22(1): 45-50.
https://www.ncbi.nlm.nih.gov/pubmed/15083380
(1d) . Treatment of severe postmenopausal endometriosis with an aromatase inhibitor. Fertil Steril (1998); 69: 709– 713.
https://www.ncbi.nlm.nih.gov/pubmed/9548162?dopt=Abstract
(1e) Bulun et al. Role of aromatase in endometrial disease. J Steroid Biochem Mol Biol (Dec 2001); 79(1-5): 19-25.
https://www.ncbi.nlm.nih.gov/pubmed/11850203
(2) Razzi et al. Treatment of severe recurrent endometriosis with an aromatase inhibitor in a young ovariectomised woman. BJOG (Feb 2004); 111(2): 182-184.
https://doi.org/10.1046/j.1471-0528.2003.00038.x
https://obgyn.onlinelibrary.wiley.com/doi/full/10.1046/j.1471-0528.2003.00038.x
(3) Shippen & West. Successful treatment of severe endometriosis in two premenopausal women with an aromatase inhibitor. Fertil Steril (May 2004); 81(5): 1395-8.
https://www.fertstert.org/article/S0015-0282(04)00147-5/fulltext
(4) Fatemi, Human Mousavi. Successful treatment of an aggressive recurrent post-menopausal endometriosis with an aromatase inhibitor. RBM Online (2005); 11(4): 455-457.
https://www.rbmojournal.com/article/S1472-6483(10)61140-6/pdf
SUPPORT GROUP FOR ENDOMETRIOSIS PATIENTS
There are many support groups including:
(1A) Endometriosis – Perth Sisterhood of Support.
https://www.endoperthsisters.com
Above support group is run by endometriosis sufferers, Joanne McCormick and Monique Alva (see below story).
(1B) Hedley, Kate. ‘The bad days are shocking’: Fresh hope for endometriosis sufferers. WA Today (15 Dec 2017).
